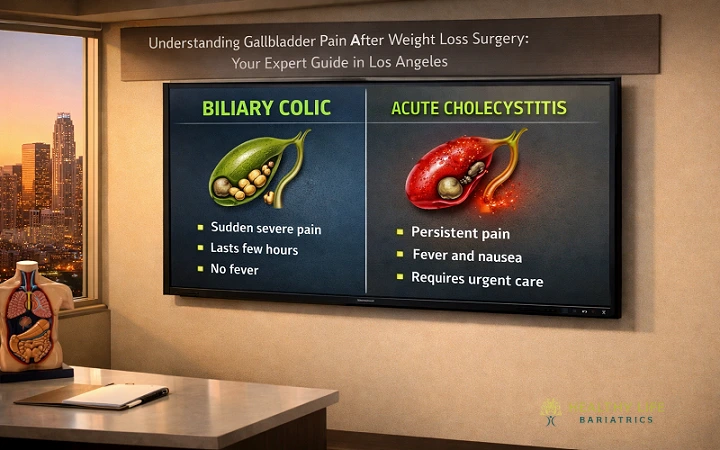
The fundamental difference between Biliary Colic and Cholecystitis lies in the duration of the blockage and the presence of inflammation: biliary colic is a temporary obstruction of the cystic duct that causes intermittent pain, while cholecystitis is a persistent, inflammatory infection caused by a permanent blockage that requires immediate medical intervention. While biliary colic acts as a painful warning sign that usually subsides within a few hours, cholecystitis is a serious medical crisis characterized by constant pain, fever, and potential gallbladder wall damage.
In this guide, we will dive deep into the pathophysiology, symptoms, and treatment options for both conditions, with a special focus on why these issues are prevalent after rapid weight loss.
In order to understand the causes of such malfunctioning, it is necessary to be aware of what normal gallbladder function involves. The gallbladder is a small sac shaped like a pear located below the liver. It mainly acts as a storage for bile produced by the liver.
When food is consumed, particularly when fat is present, the production of a hormone known as Cholecystokinin (CCK) occurs in the small intestine. The function of CCK is to contract the gall bladder, pushing bile into the cystic duct, the common bile duct, and the small intestines.
Gallstones form when there is an imbalance in the chemical makeup of bile. This usually happens in three scenarios:
Biliary colic is the clinical term for the pain caused by a gallstone temporarily blocking the exit of the gallbladder. Think of it as a “clogged pipe” that occasionally clears itself.
When the gallbladder contracts to push out bile after a meal, a stone can get sucked into the opening of the cystic duct. This creates a sudden increase in pressure inside the gallbladder. The intense pain felt is the gallbladder’s muscle wall struggling to overcome this blockage.
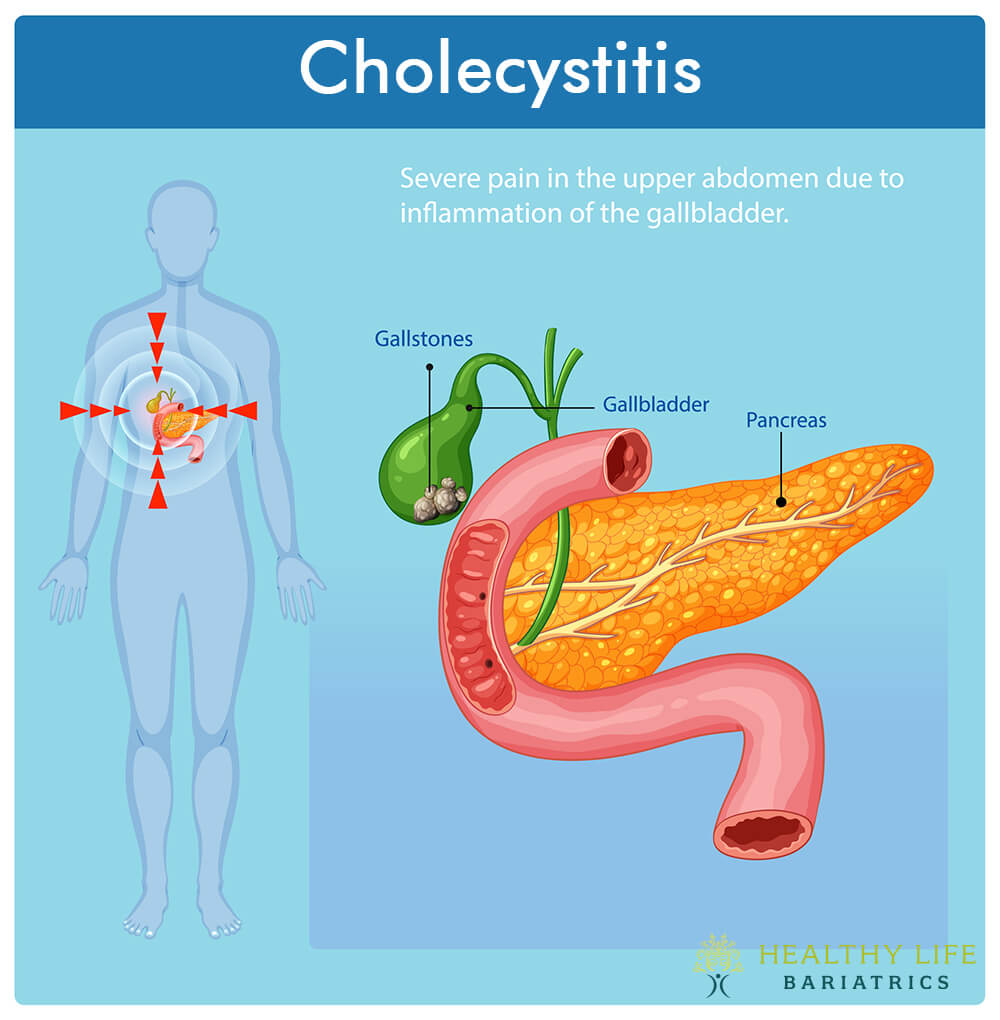
If biliary colic is a temporary blockage, Acute Cholecystitis is a persistent, inflammatory crisis. In this case, the stone does not move back into the gallbladder; it stays wedged in the neck or cystic duct.
When the duct is permanently blocked, bile becomes trapped. The trapped bile acts as a chemical irritant to the gallbladder wall. This leads to:
However, patients at Healthy Life Bariatrics Clinic are at a higher risk of gallbladder problems than the general population. The reason is that rapid weight loss can cause such complications.
As the body rapidly metabolizes fat stores, the liver releases extra cholesterol into the bile. This creates “supersaturated” bile, which is the perfect environment for gallstones to crystallize.
Weight loss surgery affects how the gut and gallbladder work together. When you eat fewer calories, your gallbladder contracts less often. This causes bile to sit longer, which can turn it into “sludge” that may harden into stones.
Research shows that the highest risk period for developing symptomatic gallstones is between 6 and 18 months post-surgery. This is why Dr. Babak Moein emphasizes monitoring abdominal symptoms during the first two years of recovery.
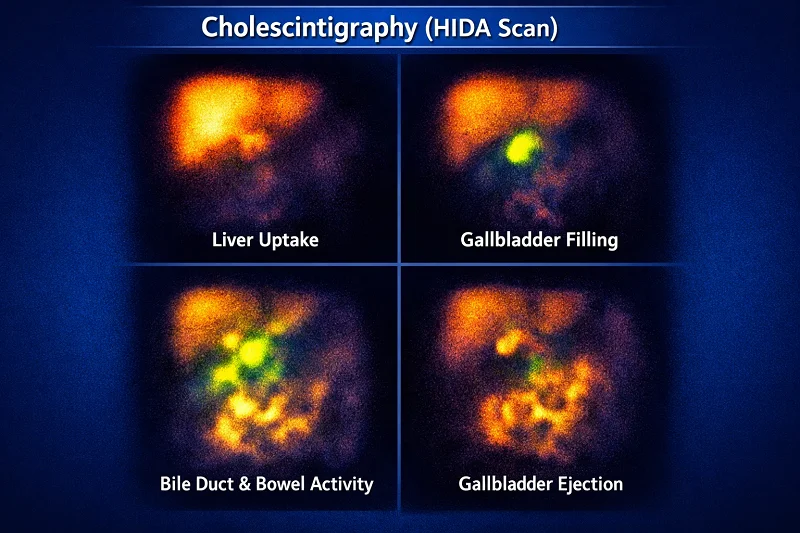
How do we tell the difference in a clinical setting?
Regardless of whether you have colic or cholecystitis, once gallstones become symptomatic, the definitive treatment is surgical removal of the gallbladder.
For very mild biliary colic, some might attempt a zero-fat diet. However, medical data suggests that 70% of people who have one attack will have another, often more severe, within a year.
Absolutely. The gallbladder is a storage tank, not a factory. Your liver will continue to produce bile, which will now trickle directly into your intestine. Most patients digest food perfectly fine after a short adjustment period.
The pain is the same, but the implications are different. Because bariatric patients have a smaller stomach “pouch,” intense abdominal pain can sometimes be confused with other post-op issues like marginal ulcers or bowel obstructions. This is why a specialized evaluation by a bariatric surgeon is essential.
In many cases, yes. Dr. Moein may prescribe Ursodiol (a bile acid) for the first 6 months post-op to help keep bile thin and prevent stone formation during the peak weight loss phase.
Your body uses pain as a communication tool. Biliary colic is a “request” for intervention; cholecystitis is a “demand” for emergency care. If you are a bariatric patient experiencing upper right abdominal pain that radiates to your back, do not dismiss it as “indigestion.”
At Healthy Life Bariatrics, we specialize in the unique needs of the metabolic patient. Whether it’s managing post-operative gallbladder sludge or performing a life-saving emergency cholecystectomy, our goal is to keep your weight loss journey safe, successful, and pain-free.
We invite you to see the transformative results of our patients by visiting our Before & After Gallery. If you are experiencing symptoms or have questions about your gallbladder health after surgery, don’t wait for the pain to escalate. Contact us online today or speak directly